What Causes Hip and Groin Pain?



Hip movement checks help guide the next step.
Hip and groin pain causes may include irritation inside the hip joint, a groin strain, tendon overload, bone stress or referred pain from the lower back or pelvis. Symptoms often appear during walking, running, sitting, stairs, squats, kicking or changing direction.
A hip pain physiotherapy assessment can help identify the most likely source. This is especially useful when hip pain overlaps with groin pain or lower back symptoms.
Quick Answer: What Causes Hip and Groin Pain?
Common hip and groin pain causes include hip osteoarthritis, femoroacetabular impingement, hip labral irritation, groin strain, adductor tendon pain, hip flexor pain, gluteal tendon pain and referred pain from the lower back.
Pain location offers clues, but it does not confirm a diagnosis. Stiffness, clicking, weakness, limping, altered sensation and activity triggers help build a clearer clinical pattern.
What Are the Main Hip and Groin Pain Causes?
Most causes fit within several broad groups: hip joint problems, muscle or tendon overload, outer hip conditions, referred pain, bone stress and inflammatory or medical conditions.
Deep pain at the front of the hip or groin can suggest involvement of the hip joint. Inner-thigh pain may involve the adductor muscles or tendons. Outer hip pain commonly relates to the gluteal tendons or nearby bursa. However, symptoms can overlap, and lower back problems may also refer pain into the hip or groin.
Deep Front Hip or Groin Pain
The hip joint, labrum, FAI or hip arthritis may contribute.
Common clues: stiffness, clicking, catching, reduced rotation, sitting pain, squatting pain or difficulty getting out of a car.
Inner-Thigh or Groin Pain
The adductor muscles or tendons are common sources.
Common clues: pain with squeezing the legs together, sprinting, kicking, cutting, lunging or changing direction.
Outer Hip Pain
Gluteal tendon or trochanteric pain may be involved.
Common clues: pain with side-lying, stairs, hills, walking, standing on one leg or lying directly on the painful side.
Back, Buttock or Leg Symptoms
Lower back referral or nerve irritation may contribute.
Common clues: burning pain, pins and needles, numbness, pain below the knee or symptoms that change with spinal movement.
Important: These patterns provide clues only. More than one structure may contribute, and pain location alone cannot confirm the diagnosis.
What Symptoms Suggest a Hip Joint Problem?
Hip joint pain often feels deep at the front of the hip or within the groin. It may worsen with sitting, stairs, hills, deep squats, twisting or getting in and out of a car.
- Hip osteoarthritis may cause stiffness, aching and reduced hip movement.
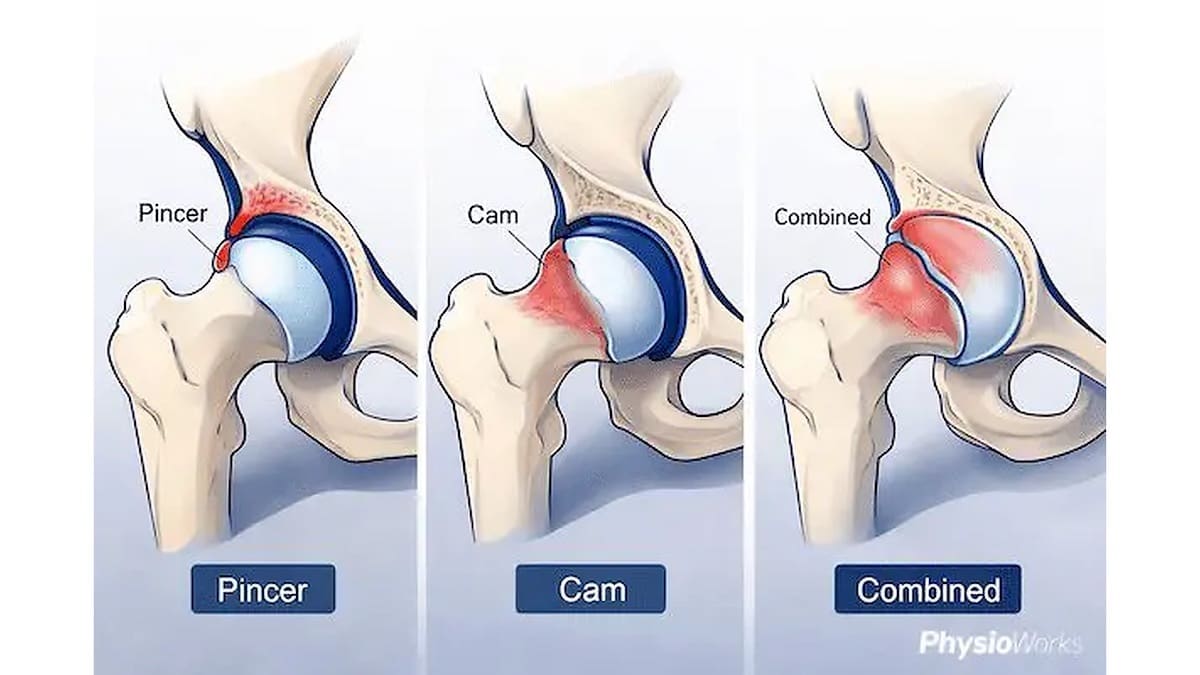
- Femoroacetabular impingement syndrome may irritate the hip during deep bending or rotation.
- A hip labral tear may cause sharp pain, clicking, catching or a blocked feeling.
- Avascular necrosis is less common but important because it affects blood flow to the femoral head.
Several joint-related problems can feel similar during their early stages. Assessment may examine hip movement, strength, walking, single-leg control and how symptoms respond to different positions and loads.
Could the Pain Come From a Muscle or Tendon?
Muscle and tendon overload is common in active people, runners, field-sport athletes and gym users. Symptoms may build gradually or begin after a sprint, kick, lunge or sudden direction change.
- A groin strain often causes sudden inner-thigh or groin pain during a high-load movement.
- Adductor-related groin pain may hurt with squeezing, running, cutting or kicking.
- Hip flexor pain may worsen when lifting the knee, sprinting or rising from sitting.
- Gluteal tendinopathy commonly causes outer hip pain with walking, stairs or side-lying.
- A broader muscle strain may follow sudden overload or repeated fatigue.
Muscle and tendon problems often respond to staged loading. However, the exercise plan should match the likely tissue, symptom level, current capacity and activity goal.

Adductor testing can help identify possible groin-related sources.
What Causes Pain on the Outside of the Hip?
Outer hip pain commonly relates to sensitivity within the gluteal tendons and surrounding tissues. Many people notice pain during side-lying, walking, stairs, hills or prolonged single-leg standing.
Care often focuses on reducing irritating compression, adjusting activity, improving hip strength and gradually rebuilding walking or running tolerance.
Can Back Pain Cause Hip or Groin Pain?
Yes. Lower back pain, sciatica and a pinched nerve may refer symptoms into the front, side or back of the hip.
Back-related symptoms may include burning pain, pins and needles, numbness, leg pain or symptoms that change when you move your spine. By comparison, hip joint symptoms often change more with hip rotation, squatting, stairs, sitting or getting in and out of a car.
What Other Health Conditions Can Cause Hip or Groin Pain?
Less common causes still require consideration. Osteoporosis may increase fracture risk. Rheumatoid arthritis may cause joint pain, swelling and prolonged morning stiffness. A stress fracture may cause deep pain that worsens with impact, running or repeated loading.
Medical review becomes more important when pain is severe, follows trauma, worsens despite rest, affects general health or prevents weight-bearing.
How Does Physiotherapy Help Identify the Cause?
A physiotherapist examines the full symptom pattern rather than relying on pain location alone. Assessment may include hip range, strength, resisted muscle testing, balance, walking, squats, steps, spinal screening and activity-specific loading.
These findings help determine whether symptoms are more likely to involve the hip joint, adductors, hip flexors, gluteal tendons, lower back or another source. They also guide load modification, rehabilitation exercise and return-to-activity planning.
Imaging may help in selected cases. Your physiotherapist may recommend GP review, medical assessment or imaging when your history or examination findings suggest this is appropriate.
Should You Keep Exercising?
You may continue comfortable movement when symptoms remain mild, settle quickly and do not worsen later that day or the next morning.
- Keep walking if pain does not build or cause limping.
- Reduce painful sprinting, kicking, cutting or jumping.
- Modify deep squats if they reproduce hip or groin pain.
- Restart strength work gradually rather than testing maximum loads.
- Arrange an assessment if symptoms repeatedly return.
When Should You Seek Help?
Book an assessment when hip or groin pain lasts more than a few days, limits walking, causes limping, stops sport, affects sleep or returns whenever activity increases.
Seek urgent medical care if you cannot bear weight, have major trauma, fever, severe or worsening night pain, unexplained weight loss, sudden testicular pain, significant abdominal pain or severe pain with feeling generally unwell.

Guided control and progressive loading support a safer return to activity.
What To Do Next
If hip or groin pain limits walking, work, training or sport, consider a physiotherapy assessment. Early guidance can help identify the likely source, reduce repeated flare-ups and support a safer return to normal activity.
For athletes and active adults, assessment may also guide training changes, strength progression and return to running, kicking, cutting or gym exercise.
Related Hip and Groin Information
Start With the Main Guides
Hip Joint Conditions
Muscle and Tendon Problems
Returning to Activity
Hip and Groin Pain FAQs
What causes hip and groin pain?
Hip and groin pain may come from the hip joint, nearby muscles or tendons, bone stress or referred pain from the lower back or pelvis. Common triggers include walking, running, sitting, stairs, squats and twisting.
Can hip pain cause groin pain?
Yes. Hip joint problems may refer pain into the groin. This can occur with hip arthritis, femoroacetabular impingement and hip labral irritation. Symptoms may worsen with sitting, squats, twisting, stairs or getting in and out of a car.
What does adductor-related groin pain feel like?
Adductor-related groin pain often feels like inner-thigh or groin pain. It may worsen with sprinting, kicking, cutting or squeezing the legs together. Symptoms may begin suddenly or build gradually with repeated loading.
When should I see a physiotherapist for hip or groin pain?
Consider an assessment if pain lasts more than a few days, limits daily activity, affects walking, causes limping, stops sport or repeatedly returns after rest.
Can exercise help hip and groin pain?
Exercise may help when it matches the likely cause and stage of pain. Rehabilitation may include hip, groin, trunk and leg strengthening followed by gradual progression of walking, running, stairs or sport tasks.
Choose your clinic and appointment pathway
Select a PhysioWorks clinic to continue to live booking, an appointment request or reception assistance.
Hip Products
These hip products are commonly used by our physiotherapists to improve strength, posture, movement, plus assist home exercise programs.
-
 Ankle, Back, Braces & Supports, Calf, Foot, Groin, Heel, Hip, Knee, Thigh, Walking
Ankle, Back, Braces & Supports, Calf, Foot, Groin, Heel, Hip, Knee, Thigh, WalkingForearm Crutches
$64.00Select optionsQuick View - Exercise Equipment, Resistance Band
POW.R Wide Fabric Loop Resistance Band
$14.95 – $49.95Select optionsQuick View -

 Exercise Equipment, Resistance Band
Exercise Equipment, Resistance BandAllCare Powerloop Bands
$22.00 – $65.00Select optionsQuick View -


-


-


-


-


-
 Exercise Equipment, Knee, Resistance Band
Exercise Equipment, Knee, Resistance BandPOW.R Fabric Mini Loop Bands
$12.00 – $55.00Select optionsQuick View -


-

 Exercise Balls, Back, Exercise Equipment, Knee, Shoulder
Exercise Balls, Back, Exercise Equipment, Knee, Shoulder66fit Exercise Balls | Core & Rehab Stability Ball
$32.00 – $57.00Select optionsQuick View -
-


-
- Liniments & Gels, Massage Liniments, Pain Management
Fisiocrem
$16.95 – $39.95Select optionsQuick View -





References
- Reiman MP, Thorborg K, Hölmich P, et al. Consensus recommendations on the classification, definition and diagnostic criteria of hip-related pain in young and middle-aged active adults from the International Hip-related Pain Research Network, Zurich 2018. Br J Sports Med. 2020;54(11):631–641.
- Rolph R, Morgan C, Chapman G, Marsh S. Groin pain in athletes. BMJ. 2020;368:m109.
- Short SM, Tenforde AS, Lau B, et al. Hip and groin injury prevention in sport. Int J Sports Phys Ther. 2021;16(1):172–183.
- Martins TB, Nunes GS, Freitas-Júnior IF, et al. Risk factors associated with groin pain in athletes: a systematic review with meta-analysis. Life (Basel). 2025.