Hip impingement can cause deep front-of-hip or groin pain. It may feel like a pinch, catch or block during squats, sitting, running, kicking or twisting. It often overlaps with other causes of hip pain and groin pain, so a clear assessment helps guide the right plan.
Clinicians often use the term Femoroacetabular Impingement Syndrome, or FAIS. This means your symptoms, clinical signs and imaging findings fit together. Hip shape alone does not prove FAIS, because some people have cam or pincer shapes without pain.
Quick answer: hip impingement often causes a deep groin or front-of-hip pinch during deep bending, twisting, sport or long sitting.
Next step: assessment checks whether symptoms fit FAIS, a hip labral tear, hip flexor pain, adductor overload, back referral or early joint change.
What Is Hip Impingement?
Hip impingement happens when the ball and socket of the hip come into early contact during movement. This contact most often occurs when the hip moves into deep flexion and rotation.
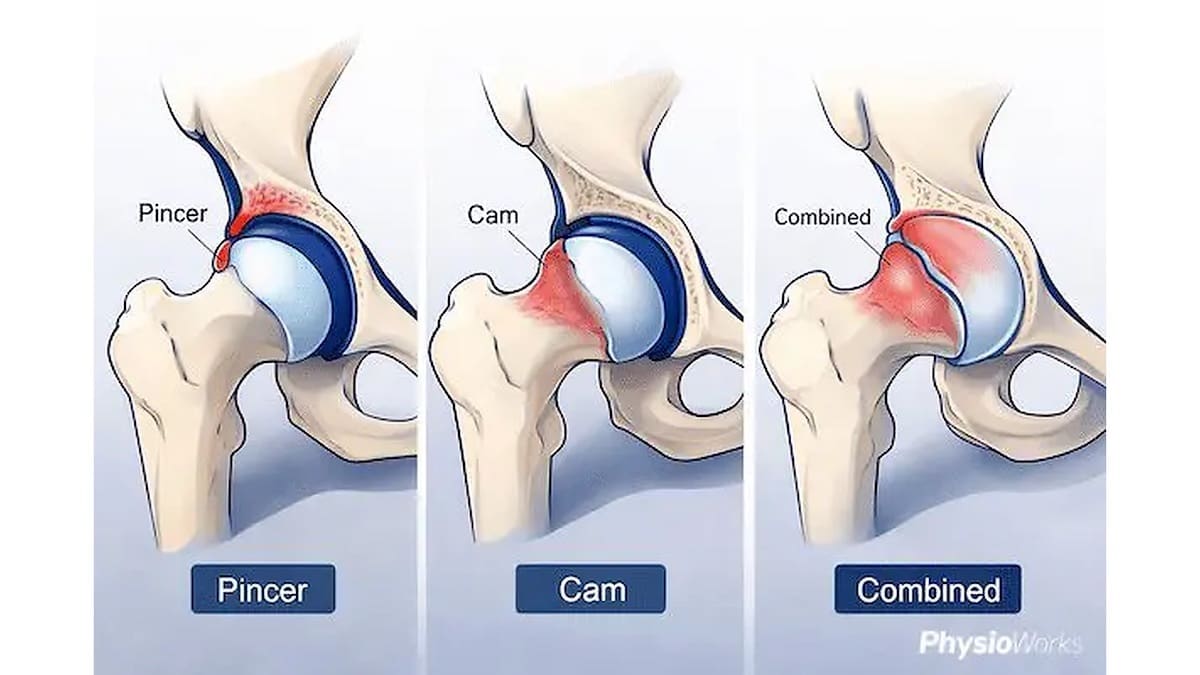
The hip may have a cam shape, a pincer shape or both. These shape features can increase contact between the femoral head-neck junction and the socket rim. This may irritate the labrum, joint surface and nearby tissues.
Still, structure is only one part of the picture. Pain, movement, strength, training load and daily positions all matter.
Common Signs of Hip Impingement
deep groin or front-of-hip pain
pinching with squatting, lunging or sitting low
reduced hip range, especially flexion or rotation
clicking, catching or a blocked feeling
pain with running, kicking, pivoting or gym training
Hip impingement usually relates to a mix of hip shape, repeated loading and movement demand. Symptoms may start when training rises, hip control drops, squat depth increases, or sport loads the hip into deep flexion and rotation.
Primary causes often relate to hip development and long-term loading patterns. This is one reason active people and athletes may notice symptoms. Secondary causes may follow previous hip problems or structural change, such as Perthes disease or a previous fracture around the hip.
Hip impingement can also overlap with hip flexor pain, hip adductor tendinopathy, hip labral irritation and lower back referral. Pain location alone is not enough.
What Are the Types of Hip Impingement?
Pincer, cam and combined hip impingement types.
There are three common patterns:
Cam impingement: extra bone at the femoral head-neck junction can reduce smooth motion.
Pincer impingement: extra coverage from the socket rim can increase contact at the front of the hip.
Combined impingement: cam and pincer features both contribute to early contact.
Many people have mixed features. The key question is whether the shape, symptoms and clinical tests all match.
How Is Hip Impingement Diagnosed?
Hip impingement is diagnosed using symptoms, physical tests and imaging where needed. Scans alone are not enough. Some people show hip shape changes without pain.
Your physiotherapist will ask which movements provoke symptoms. They may check whether the hip clicks, catches or feels blocked. They will also ask whether sitting, stairs, squats, running or sport make pain worse.
Assessment usually includes hip range testing, strength testing, movement control checks and provocation tests. These tests aim to reproduce your familiar symptoms. X-rays may help assess hip shape when FAIS is suspected. MRI may help when a labral tear, cartilage injury or another joint problem is being considered. For a broader clinical overview, see the clinical practice guideline for non-arthritic hip pain.
Assessment Usually Checks
hip flexion and rotation range
pain during squat, lunge, step or sitting positions
hip, pelvis and trunk strength
clicking, catching, locking or giving way
overlap with groin, back or outer hip pain
Hip Impingement Treatment
Most people start with non-surgical treatment. Physiotherapy aims to reduce pain, improve useful hip mobility, rebuild strength and improve hip, pelvis and trunk control. This helps the joint handle load with less repeated pinching.
Early activity changes often help. This may mean reducing deep squats, changing sitting breaks, adjusting running volume, modifying kicking load or changing gym depth for a short time.
A rehabilitation plan may include manual therapy, strength work, movement retraining and a gradual return to sport or gym tasks. Your physiotherapist may also help you adjust training volume, exercise technique and loading speed. For broader context, see our physiotherapy and common physiotherapy treatment techniques pages.
Can You Keep Exercising?
You may keep exercising if symptoms stay mild, your walking stays normal, and pain settles quickly after activity. However, sharp pinching, limping, night pain or worsening next-day stiffness means you should scale back and seek advice.
Hip Impingement Load Guide
Usually okay
Walking, easy cycling, light strength work and shallow range exercise if symptoms stay mild.
Modify
Deep squats, heavy lunges, sprinting, kicking, pivoting and long sitting if they trigger pinching.
Book assessment
Repeated flare-ups, limping, catching, locking, night pain or loss of range.
When Is Surgery Considered for Hip Impingement?
Surgery may be considered when symptoms remain limiting after a well-guided period of rehabilitation and load change. This is more likely when pain affects work, sport, daily function or sleep, and when clinical findings and imaging support hip impingement as the main driver.
Hip arthroscopy is the most common surgical approach. It may address the bony impingement pattern and, where needed, associated labral or cartilage problems. Surgery is not the first step for most people, so conservative care is usually tried first.
Seek medical care quickly if hip pain follows major trauma, you cannot bear weight, you feel unwell with fever, pain is severe at night, or symptoms are rapidly worsening.
What to Do Next
If your hip feels pinchy, stiff or painful with loaded movement, a physiotherapy assessment can help clarify whether hip impingement is likely. It can also check whether another hip or groin condition is contributing.
A clear diagnosis matters because treatment should match the structure involved, your activity goals and the movements that trigger symptoms. Many people improve with education, load change, hip strength work, movement retraining and a graded return to activity.
Hip impingement often feels like a deep pinch at the front of the hip or groin. It may worsen during squats, lunges, sitting low, running, kicking or twisting. Some people also notice stiffness, clicking, catching or a blocked feeling.
Is hip impingement the same as FAIS?
Hip impingement is the common term. FAIS, or Femoroacetabular Impingement Syndrome, is the clinical term when symptoms, physical signs and imaging findings fit together. Hip shape alone does not confirm FAIS because some people have shape changes without pain.
Can hip impingement improve without surgery?
Yes. Many people start with physiotherapy, load change, strength work and movement retraining. The goal is to reduce repeated painful pinching, improve hip and pelvis control, and rebuild activity tolerance. Surgery is usually considered only when symptoms remain limiting despite a clear rehabilitation plan.
Should I stretch hip impingement?
Gentle mobility may help some people, but forceful stretching into a painful pinch can irritate symptoms. Many people do better with a mix of activity changes, hip strength, trunk control and careful range work. Your assessment should guide which movements suit your hip.
When should I get imaging for hip impingement?
Imaging may help when symptoms persist, the diagnosis is unclear, or a labral or cartilage problem is suspected. X-rays can assess hip shape. MRI may help assess soft tissues. A physiotherapist or doctor can advise whether imaging is needed.
Can I run with hip impingement?
You may run if symptoms stay mild, your walking or running gait stays normal, and pain settles after training. Reduce speed, hills, stride length or volume if symptoms build. Stop and book an assessment if you limp, lose range, or symptoms keep flaring the next day.